|

 |  |
|
| |
 | Alimentatie | Asistenta sociala | Frumusete | Medicina | Medicina veterinara | Retete |
Aspects of the osteo-musculo-articular over use' s pathology in he pianistic activity
Recent studies at the European and American level, indicate an important increase of the frequency of the osteo-muscular-articular system's disorders caused by exercising a profession. An exaggerated over use of different segments, especially at the level of the superior member, by increasing the amplitude of movements, the repetitivity of gestures, the maintenance of some vicious positions, leads to a significant multiplication of the affections at this level, including them in the first positions of professional affections. The nerves, tendons, tendinous sheaths and the muscles of the superior member are the most affected structures by the disorders occurred after cumulative traumatisms [1, p.1].
The accumulations in the quality plan, the increase of the demandings and the tendency towards performance in every domain, phenomena that characterize the last decades of the XXth century, have had echo also in the instrumental musical education. On all steps of the piano training, the competition, as a factor of values' sorting, is more and more fierce. This enthusiasm trains towards performance not only the pupils and over-endowed pietistic students but also the ones with a medium technique and musical endowment, which make consistent efforts, sometimes over dimensioned, in order to face the imposed exigencies. Among them, the ones less resistant to effort would be predisposed to hand, arm and spine's over use diseases.
The musculo-articular over use
In a professional activity the over use expresses the excess of effort imposed to some segments or systems of the organism that overtakes the normal functional capacity of them.
Liviu Pop defines the term over use as being "the cause of an aberrant answer of the human biological system at the physic-psychical and biomechanical demands, particular to the execution of an over dimensioned professional prostration".[1, p.5]
The names of "pathologie d' hypersollicitation", "over use syndrome" or "over use injuries" from the specialized terminology, capture globally this complex phenomenon, and can be applied at every type of injuries met in the osteo-musculo-articular pathology.
The affections of the pianistic device due to the over use in the study of the piano, can be included in this category of professional diseases of the osteo-musculo-articular system.
At this point we talk about an excess of effort which overtaking the normal physical resources, at a time, of the piano player, develops affections or even diseases of the segments of the pianistic device.
In the activity of piano studying, the over use can develop in two directions. On one hand it produces through a sudden and exaggerates increase of the number of hours of study. The organism, not being adapted to the created situation answers by getting ill. On the other hand, the over use can appear in case of insistent study of some technical formulas of high difficulty. It thus appears an excessive demand of the same articulations and groups of muscles, that leads to the over tension of the area.
In both cases a passing of the limit between physiological tiredness and pathological tiredness produces.
The physiological tiredness is a normal process that appears after a physical activity - in our case, the piano study - that trains some musculo-articular segments of our body. If the effort is correctly dosed, the organism has the resources that are necessary to the recuperation in that plan.
The pathological tiredness appears when the effort is over dimensioned, the activity, is repeated obsessively, before having the opportunity of recuperating the segments trained in the action [2, p.147]. The acute form of pathological tiredness is the over tension that represents the discordance between request and the answering capacity of the organism.
In the piano study, the over tension, as an effect of the over use, is characterized by muscular discomfort, stiffness or even painful muscular contracture. This is the first signal that warns over a possible slip towards disease.
The excessive demand by studying the piano, without recuperation breaks of the musculo-articular potential, can lead to real diseases of the hand, arm, shoulder. Morphological and functional modifications appear at the level of these segments, inflammatory processes of mechanical nature localized at the level of articular insertions appear.
Through a correct organization of the piano study, referring to the time and intensity of the demands in technical plan, the emergence of these situations is avoided. The detection of the smallest likely signs of getting to the pathological thresholds of tiredness is also important. In these cases, the breakdown of the piano study is necessary in order to restore the functional capacity of the pianistic device.
The causes and conditions that favor the trigger of the affections of the pianistic device1 are multiple and varied. Of them we can name: deficits in the general health status of the piano player (lack of calcium, magnesium), hereditary predispositions towards diseases of the osteo‑musculo‑articular system, a frail habit that determines the incapacity of supporting a long, intense effort. Also, the physical construction of the arm and hand, less according with the pianistic activity - an insufficiently developed arm compared with the waist, a small hand, with rigid or too relaxed musculature, short fingers, rigid or long, but with exaggerate flexibility and with low muscular force- are conditions that favor the installation of affections at this level.
There are also subjective causes that release the diseases regarding the process of pianistic training and the daily piano study: deficient positions of the body and arms at the piano, the inefficacy of pianistic movements, the over dimensioned study regarding the number of hours, the approach of difficult repertoires that are over the technical possibilities of the piano player. These situations can be avoided through a careful surveillance of pupils' pianistic activity by the teacher. From the category of the trigger conditions of the pianistic device diseases we will select some aspects met more often.
Deficient positions of the body and hand at the piano
The efficiency of movements represents one of the most important factors that assures the progress in the pianistic technique development. It implies the inverse ratio rapport between the laid‑down effort (minimum) and the obtained efficiency (maximum). Ignoring this aspect leads to the assimilation of some noneconomical pianistic movements, clumsy and uncomfortable gesture that affect not only the technical development but also the artistic fulfillment in interpretation.
The starting point of assimilating some efficiently functional movements is the appropriation and consolidation, in the first years of study, of a correct and natural position of the body and hand at the piano.
The position of the body at the piano. In appropriating a correct position at the piano there are a few generally valid demandings, but that must not be absolutized. The correct position at the piano is individually decided, depending on the pupil's waist and his arms' length. The teacher will indicate the best distance from the piano that allows freedom in the arm movements on the whole keyboard, and then will explain which the natural position at the piano is: straight back, easily inclined towards the keyboard, the arms away from the body, sustained from the shoulders and supported on the fingertip on the key (fig.1).
 For a
little pupil, that doesn't touch the floor with his feet, the use of a little
chair for legs is necessary, in order to obtain a maximum stability. The pupils
endowed with a "natural" of movements will quickly find the comfortable
sensation in front of the keyboard. The most frequent deviations from the
general accepted formula of the correct position appear because of the modification
of the back position. This comes from the incomplete development and sustaining
of the muscles from the lombar part of the spine. The deficient position
resulted is manifesting by the exaggerate emphasizing tendency of the dorsal
and lombar curve of the spine.
For a
little pupil, that doesn't touch the floor with his feet, the use of a little
chair for legs is necessary, in order to obtain a maximum stability. The pupils
endowed with a "natural" of movements will quickly find the comfortable
sensation in front of the keyboard. The most frequent deviations from the
general accepted formula of the correct position appear because of the modification
of the back position. This comes from the incomplete development and sustaining
of the muscles from the lombar part of the spine. The deficient position
resulted is manifesting by the exaggerate emphasizing tendency of the dorsal
and lombar curve of the spine.
Fig. 1
The great attention that must be given to this aspect stands in the risk of emergence, by persevering in vicious positions, of the spine's deformations (cifoza, scoliosis, lordosis).
Another unnatural position of the body at the piano appears because of withdrawing too early the support for the legs, the little chair. Usually the chair is withdrawn in order to use the piano's pedal. The pupil heavily reaches the pedal, and because of this, extending the leg to reach it, the body leans towards backwards.
The center weight thus moves out of the arms' activity space, resulting the impossibility of using the natural weight of the arm (fig 3).


Fig. 2 Fig. 3
Also, an inadequate distance from the piano's keyboard can generate mistakes in the natural position of the body. Getting too close, the arm's action space restricts, thus limiting the movements ease over the keyboard (fig 4); an exaggerate distance from the keyboard favors the rounding of the back and the installation of an instability of the body, which is forced through bending to find a support especially in fingers (fig 5). This position also determines an excessive request of the fingers, hand and forearm's musculature.


Fig. 4 Fig. 5
These vicious positions can be corrected easily, if they are noticed in time. The permanent sense of observation of the teacher is necessary in order to detect the smallest deviations from the natural position at the piano and from the concern of eliminating them.
The placement of the hand on the keyboard. In establishing a natural position of the hand on the keyboard, the teacher won't impose to the pupil a fix, rigid position, but depending on each conformation will indicate a placement which to allow the obtaining of a maximum mobility in making pianistic moves. One cannot talk about a fix standard position of the hand while in the execution itself, the hand and fingers are in a permanent move. The general indications as "vaulted palm, easily arched fingers" serve as a landmark of the correct position of the hand, and adapt at every hand's conformation. The teacher's role is to observe the characteristics of pupil's hand conformation and to help him find the most natural and simple moves.
If the term of "correct position" of the hand's placement on the keyboard is an elastic notion, there is, however, through exaggerate deviations from it, the possibility of emergence of some vicious positions, harmful, which prevent the development of the natural in pianistic moves. The most frequent positions are manifesting at the level of the palm, by dropping it's vault (fig 6) or bending the whole hand towards the finger five (fig 7), both having as a result the breakdown of the energetic flow that can be sent from the shoulder and arm to the fingertip.
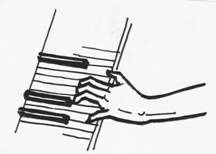
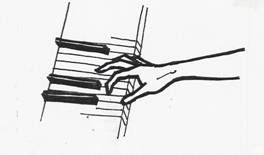
Fig. 6 Fig. 7
At the level of the fingers, vicious positions can appear which prevent the achievement of hand's stability and sustaining the weight of the arm on the fingertips. They appear at the level of the last phalange of fingers, by the exaggerate slip towards interior or exterior (fig 8a, b).
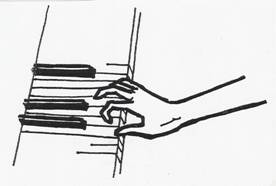
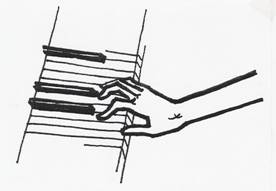
Fig. 8a Fig. 8b
These deviations from the natural position appear because of the insufficient development of the hand musculature at young ages. They can be corrected through exercise which should develop hand's muscles and consolidate the position of the hand on the keyboard.
Regarding the poignet's joint, a correct development of the pianistic technique assumes obtaining a maximum mobility of it, in order to dispose the hand against the forearm and arm in the most appropriate positions in making some natural moves. Through gentle moves, of rotation or running, it passes through many intermediate positions which ensure the natural bond between hand and forearm. The obtaining of a sensation of suppleness of the poignet must be followed from the first exercises with the beginning pupil, in order to avoid him becoming tensionate while playing the piano and to avoid possible vicious positions (fig 9a,b).
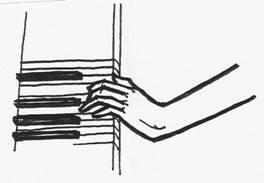
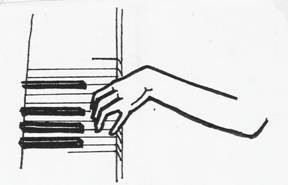
Fig. 9a Fig. 9b
The exaggerate fall and lift of the poignet while playing the piano determines, as in the case of other vicious positions, the breakdown of the energetic flow from the arm towards fingertips and prevents the pianistic device to work unitary and efficiently.
Affections of the spine
We have included in this study aspects regarding the spine, because even if it doesn't belong to the pianistic device in stricto sensu, it has an important role in the good development of the pianistic activity.
A correct and natural position of the body is given, first of all, by the spine, the bony axis of the organism [3, p. 38-47].
The most frequent deviations from the general accepted formula of the correct position at the piano appear because of the modifications of the back position. This is favored by the incomplete development and maintenance of muscles from the lombar part of the spine. The deficient position resulted is manifesting by the exaggerate tendency of emphasizing the dorsal and lombar curve of the spine.
The great attention that must be granted to this aspect, stands in the risk of emergence, by persevering in vicious positions, of spine contortions (cifozas, scoliosis, lordosis).
Seen from the front, a spine is rectilinear, any deviations could be considered pathological.
In saggital plan (profile) it presents four physiological curves (figures 10 a, b).
Fig. 10a[1]
The emphasis of these curves has pathological connotations leading to real diseases of the spine, if not observed and corrected in time.
The deformations of the spine are many, in both plans (frontal and saggital), appearing mostly as combined pathology.
From the point of view of their gravity, the spine's deformations are of two categories:
Functional deviations (vicious attitudes- cifotic attitude, scoliotic attitude) that can be easily corrected through exercice, physiotherapy, medical gymnastics
Structural deviations (structural cifoza, structural scoliosis) that represent irreducible or less reducible modifications of the curves and have a clear tendency towards aggravation (need orthopedic treatment or even surgery)
Next we will refer at the three main types of deformations that appear at the level of the spine: cifoza, scoliosis, lordosis).
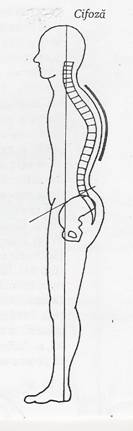
Cifoza
 Cifoza
represents the deformation through the emphasis of the posterior curve of the
thoracic part of the spine (fig 11).
Cifoza
represents the deformation through the emphasis of the posterior curve of the
thoracic part of the spine (fig 11).
The term comes from greek (gr. Kyfos= bent, hunched). Called in popular terms "round back", this affection usually installs in periods of emphasized growth of the child or adolescent, the cause being the insufficient development at the muscular level compared with the skeletal system's development. Another cause of the cifoza's installation (or only of the cifotic attitude) represents the persistence in vicious positions, that leads not only to deficiencies of the spine but also to incorrect and uncomfortable positions of the head, neck, shoulders, so to the alteration of the general posture. Maintaining this vicious posture, determines alterations at the level of the back and thorax musculature's development.
From the spine's affections, cifoza is more often met at children and adolescents who study the piano. This fact is due to adopting and maintaining an incorrect position during piano study, with the back rounded and the shoulders brought in front. Neglecting the adjustment of this position has repercussions not only over the technical-pianistic development but also over the health of the person.
Fig. 11
Scoliosis
 Scoliosis
(gr. scolios= sinuous) is the deformation in the frontal plan of the
spine. From the rectilinear disposition of the spine, curvatures towards right
or left appear (fig. 12). The causes that determine scoliosis' installation
(or scoliotic attitude) are many. The subjective ones refer, like in the
case of cifoza, at adopting and maintaining vicious positions of the body (for example
the incorrect position of the pupil while writing).
Scoliosis
(gr. scolios= sinuous) is the deformation in the frontal plan of the
spine. From the rectilinear disposition of the spine, curvatures towards right
or left appear (fig. 12). The causes that determine scoliosis' installation
(or scoliotic attitude) are many. The subjective ones refer, like in the
case of cifoza, at adopting and maintaining vicious positions of the body (for example
the incorrect position of the pupil while writing).
There are many causes of structural-anatomic nature or functional disorders that favor the evolution towards disease.
In the musical-instrumental education, scoliosis appears more often at the violinists, because of the asymmetrical posture of the spine up against the vertical axis, during the study.
Under the form of combined pathology, cifo-scoliosis can install at the level of the spine deformation in which the scoliotic lateral deviation is associated with a cifotic saggital one.
Fig. 12
Lordosis
 Lordosis
(gr. Lordos=curved) manifest in saggital plan, through the exaggerate
emphasis of the anterior curvature of the lombar vertebra (fig. 13).
Lordosis install, generally, after some inflammatory rheumatic processes or
after some degenerative processes at the level of the spine.
Lordosis
(gr. Lordos=curved) manifest in saggital plan, through the exaggerate
emphasis of the anterior curvature of the lombar vertebra (fig. 13).
Lordosis install, generally, after some inflammatory rheumatic processes or
after some degenerative processes at the level of the spine.
Regarding the activity of the pianistic device from a biomechanical point of view, the spine represents the "pillar" that supports all its components. The impact of the potential affections because of a constant and long pianistic activity is different at the level of its four parts. The most predisposed area at attritions is that of the cervical column, but, because of the implied sedentariness in the piano study, affections at the dorsal and lombar level can appear, especially by cumulating some micro injuries that, in time, would lead towards spondylosis.
Especially the assistant piano players, after a long period of activity (15-20 years) are exposed to the risk of lombar spondylosis' installation that appears because of the compaction of this area's vertebra. A deformation of the spine at this level can be observed, accompanied by muscular contractures, pain and limitation of movements. Next to the initially localized pain in the lombar area, in time painful irradiations can appear on the main run of the sciatic nerve.
Fig. 13
Within these three types of spine's deficiencies we have briefly referred at the causes that determine their emergence. We must specify that the causes of vertebra deviations are complex, implying congenital, metabolic, neuromuscular and posttraumatic factors, and domain of strict medical specialty, in which we hadn't entered.
Affections of the pianistic device
Microtraumatisms - prestage of deseases. The term - "microtraumatism" hasn't entered yet, in the true meaning, the attitude of diagnosis and treatment of muscle‑articular diseases. In the last years, the medical technique regarding nuclear magnetic resonance (RMN) has got into the intimacy of the processes of aggregation of micro traumatisms, processes that precede the structural anatomic alterations [4, p.80].
We'll try a concise description of mechanisms that trigger their release.
The anatomic formations pass, normally, through a physiological process of attrition which is compensated by one of cellular regeneration. When between the processes of attrition and those of regeneration takes place an imbalance against regeneration, the process of attrition, initially physiological, receives pathological connotations. There appear functional disorders, with modifications in the intimate structure of cells. If the attrition phenomena overtake those of regeneration, there takes place a pathological process of attrition, this leading to the release of micro traumatisms.
Nicolae Stanescu synthetically defines "micro traumatisms are injuries of over use induced by traumatic agents of small intensity, but repeated frequently, which overtake the potential of regeneration of tissues in cause and which generate anatomic micro injuries." [4, p.80]
The factors that generate these micro injuries are traumatic agents characterized by two aspects: small intensity and big recurrence. These traumatic agents appear after a long affectation of some monotype movements.
In the pianistic activity, micro traumatisms, at the level of the hand, especially, pass without being observed. Precursory to the functional impotency of the pianistic device that embarrasses the study at the piano, appear some small painful flares or muscular tiredness sensations that are, usually, ignored. These are the first signs of overtaking the limit between the physiological tiredness and the pathological one. If one insists with the study in these conditions, there appears the over tension - high form of pathological tiredness, which, also neglected, can lead to real diseases - muscular cramp, tendinitis, epicondylitis.
The study is not interrupted, so the process of regeneration of cellular attrition cannot be fully realized. The persistence in time (months, years) of these phenomena determine their apparition, aggravation and becoming chronically.
Generally, these micro injuries appear at the level of articular formations affecting tendons, ligaments, capsules, cartilages and so on. Small compressions, but frequent, at the level of articular surfaces generate edemas of cartilages, followed by the erosion of the bony tissues nearby or they can even become necrotic.
Usually, micro traumatic affections appear during childhood and adolescence at bones insufficiently grown-up. Also, they can be located at the growing cartilages or at the ossifications nucleus.
The first sign of micro traumatisms' manifestation at the pupils studying the piano is an easy muscle-articular discomfort. If that evolves towards pain or swelling of the area, it is necessary for the study to be interrupted (the pain is in strict connection with the recurrence of the micro traumatism). It is necessary that the person overseeing the pupil's study (teacher, parent) to make the distinction between dysfunction, as a short, passing manifestation of discomfort, which allows the continuation of the study and the signs of organic affectation which determine a long functional impotency - pain, redness and hyperemia of the area, swelling, to prevent the installation of real diseases like tendinitis, ligamentita, epicondylitis.
Invisible at the surface and neglected, without some major pathological manifestations, the accumulation of micro traumatisms at cellular level, during long periods of time, produces evolutions towards real affections.
The muscular cramp. The term "cramp" defines an involuntary contraction of a muscle or group of muscles, painful, short and with a spontaneous come back at the normal. It is a type of phisiological contraction that appears especially at the leg muscles, determined by cold, tiredness, bad circulation because of unconfortable positions [1, p.127].
The installation of the cramp is due to the decrease in the supply of the musculature with oxygen and glucose and accumulation, in surplus, of lactic acid.
The muscular cramp with pathological connotations refer to the painful contraction appeared after an activity that implies monotype movements, frequently repeated over long periods of time. This type of cramp, particular to some occupations (writer, player, typist) is defined by Doctor Liviu Pop as an "occupational cramp of the hand" [1, p.127], that appears after a repeated request at the level of it. It can be preceded by pain or sensation of muscular tiredness.
In the pianistic activity, the muscular cramp appears after a very long study, or after insistently trying to solve some technical difficulties. It thus produces an over use at the level of the hand's musculature, and overtaking the threshold of pathological tiredness determines the installation of the over tension. Physically, it develops under the form of involuntary contraction of the flexor or extensor muscles of the hand.
The first measure (imperative) to come back to normal is to stop the study at the piano and to use some positions and gestures which should not maintain or worsen the affection (the request of the affected muscles in another type of activity).
In the pianistic activity, they install most frequently at the level of the hand and of the hand's wrist (poignet).
Tendinitis is the tendon's affection caused by the inflammation of its membranes. The tendon's membranes are formed from a very delicate tissue which makes the tendon's slip movement easier. One of the reasons of membranes' inflammation is their irritation due to the articulation's over tension. The long use of the same type of movement, without the necessary brakes for the cellular regeneration, determines, at the beginning, the irritation and then the swelling of the tendinous membranes. The installed inflammation straitens the space through which the tendon slips, causing rigidity and pain at the level of the area.
Next to the over tension, other conditions that favor tendinitis' installation are: circulation disorders, endocrine disorders, wrong biomechanical skills (noneconomic movements, aggravated in the case of piano players) the study in tiredness conditions.
Tendinitis is clinically expressed by local pain (sometimes radiated) and contortion of the area under the form of a swelling of different sizes. Trying to passively or actively stretch the tendon is very painful or even impossible.
Tenosynovitis is an inflammatory affection, installed at the level of the sheaths synovium which dress the muscles' tendons. The sheath synovium is an anatomic formation that contains synovium liquid. It has the role to protect the tendons and to make their slip within articular movements easier. Its swelling embarrasses and encloses the tendons' movement.
The region of the hand's wrist is crossed by many sheaths synovium, afferent to the hand's muscles tendons. At the level of the hand's wrist we can observe three groups of tendons, with their sheaths synovium- flexor tendons, extensor tendons and sidelong tendons. The swelling of the sheaths of these tendons causes pain, a sensation of numbness and tingling at the level of the flexor and extensor muscles of the hand (the hand's flexor and extensor tenosynovitis).
The causes that favor and trigger the tenosynovitis are alike those of tendinitis: causes of micro traumatic nature - by over tension and metabolic causes.
There are two clinical forms of this affection: acute tenosynovitis and chronically tenosynovitis.
In the acute form of the affection, the area of the tendon is tumefied, reddened and painful when making moves. The palpation indicates one or more painful spots at the level of the affected tendon. Also, the area is warm and presents fluctuenta because of the sheaths synovium with edemas.
By treatment, the synovium liquid can fully or partially resolve, forming adhesions, in this case getting to the chronically form of the disease. The chronical tenosynovitis is characterized by the presence of a permanent pain, exacerbated at any request. The swelling is smaller but harder and the tendon, most of the times, feels bold, irregular.
The main therapeutic measure that imposes in the case of tendinitis and tenosynovitis is to put in absolute rest the affected tendon and even to immobilize the hand, to put the tendon in a relaxed position.
Bursitis [5, p. 1186] is an anatomic formation formed from a closed sack whose halves are invigilated one another, containing a small quantity of liquid which permits the slip. Bursas are placed next to articulations or where the skin, tendon or muscle slips over a bony prominence. They have the role of cushioning the friction between the bony plan ant the other joined anatomic elements, making the articulations' movement easier.
Like in the case of sheaths synovium, the bursas can swell under the action of an over tension, or some direct traumatisms. Their swelling determines bursitis. It produces the congestion of the bursa's walls, hyper secretion of liquid and sediments of fibrin on the membranes that line it. Thus, the role of cushioning the friction of anatomic structures between which the bursa is disposed is a lot diminished.
The clinical manifestations appear under the form of swelling and pain in the affected area, with irradiation - sometimes - over the joined areas.
Like tenosynovitis, bursitis has, from the evolution point of view, two forms - acute and chronical.
The acute bursitis is characterized by spontaneous pain, the limitation of movements and, at the level of superficial bursas (the elbow, for example) swelling and redness.
The chronical bursitis install after many episodes of acute bursitis or after repeated traumatisms. It generates thickenings of the bursa's walls and at the interior appear adherences and even calcifications. The movement of the joint is mostly limited.
In the pianistic activity, bursitis can appear at the level of the elbow after an over tension through inappropriate movements that lead to irritations and the swelling of the bursa around this joint.
Epicondylitis [1, p.92] is an affection at the level of the epicondyl- the lower part of the humerus joint (the top of the elbow) - on which the muscles of the forearm insert. The simple epicondylitis, or tendinitis of insertion of epicondyliens muscles, represents the classic form of elbow tendinitis. It appears as a manifestation of a professional over tension (or nonprofessional) of the epicondyliens groups of muscles, as a result of making some repetitive movements of the hand's wrist or fingers.
The main clinical manifestation is the emergence of pain at the elbow's level, during or after a challenging activity, pain felt under the form of an exacerbate muscular tension.
A frequent form of epicondylalgy is side-humeral epicondylitis (tendinitis of the extensor's common origin of fingers) affection known under the name of "tennis men' elbow" because it appears more frequently between tennis players. It also appears at other professional categories like piano players, as a result of performing some repetitive movements in which the extension of the hand and fingers is implied. At this type of epicondylalgy, the pain can appear not only at the level of the elbow but also at the dorsal face of the forearm, and the symptoms persist during rest and during the night.
The risk of this affection's emergence is determined by some factors - first of all professional - and grows as you get older. Epicondylitis appears as an acute manifestation, but because it presents a big probability of becoming chronical, an energetic treatment is imposed after the first flare.
We have proposed to realize our foray in the field of osteo-musculo-articular affections with possible impact on the pianistic activity, without the intention of exposing details of medical specialty. We have wished to report the possible risks of diseases of the pianistic device determined especially by the subjective causes related to the pianistic education process and the approach of piano studying. In this respect, we have emphasized the idea of the complex mission and the great responsibility of the piano teacher in guiding his pupils. On a fair knowledge and assessment of the individual physical and psychical capabilities, he can foreshadow plots of technical-musical development and progress at the level of each of them. Ignoring this aspect and overloading with tasks, in the technical plan, over the pupil's possibilities - desiring a rapid progress or obtaining performance by any price - has, in many cases, negative repercussions in the health plan.
We also consider important that the piano teacher must know the causes and conditions that favor the trigger of this type of diseases, in order to be able to prevent them. Noticing in time, small muscular malfunctions that precede the affection of segments of the pianistic device and taking some simple measures to eliminate them are essential in avoiding the installation of the pathological aspect.
This whole ensemble of preoccupations targets, in fact, reaching to the final purpose of the pianistic education process, achieving the symbiotic relation between the development of the pianistic technique and the maturation in the musical-artistical plan, idea expressed by the great piano pedagogue, the teacher Florica Musicescu: "Knowing how to master, to dominate the greatest technical difficulties, in order for the enunciation of the musical language to appear unimpeded, to be able to express as truthful as possible the composer's thoughts". [6, p. 87]
Bibliography
Tefas, Lucian, Pop, Liviu, The professional deseases of the musculo-skeletal system, Editura Medicala Universitara 'Iuliu Hatieganu', Cluj-Napoca, 2004
Dragan, Ioan, Sportive medicine, Editura Medicala, Bucuresti, 1994
3. Antonescu, Dinu, Obreja, Corneliu, Ovezea, Alexandrina, The correction of the spine, Editura Medicala, Bucuresti, 1993
Stanescu, Nicolae, Current sportive traumatology, Editura Stadion, Bucuresti, 1972
5. * * *, Intern medicine treaty, vol. II, Rheumatology, red. prof.dr. Radu Paun, Editura Medicala, Bucuresti, 1999
Paladi, Marta, Florica Musicescu, Editura Muzicala, Bucuresti, 1977
This paper brings into the attention of the instrumentalist musicians, especially piano players, (teachers, students, pupils) the ardent problem of musculo-articular diseases particular to the profession and the conditions that favor their trigger.
The affections of the spine (cifoza, scoliosis, lordosis) but also diseases like bursitis, tendinitis, epicondylitis or muscular cramp appear in the process of studying an instrument as a result of a bad management of the instrumental technique's activity of development. The main causes that trigger these diseases are: the musculo-articular over use as a result of an excess of effort made during the study at an instrument, the use of an improper instrumental gesture, inappropriate to the intended purpose or persevering in vicious positions of the body and arms during the study.
Keywords
Piano technique
Professional diseases
Muscular over-use
Muscular cramp
Tendinitis
plan posterior= posterior plan, zona cervicala = nape, vertebre= vertebra, convexitate posterioara = posterior convexity, zona dorsala = dorsal area, zona lombara = lombar area, zona sacrococcigiana = saccrococcygeal area, plan anterior = anterior plan, convexitate anterioara = anterior convexity, vertebra a 1-a cervicala (proeminenta) = the first cervical vertebrae (prominent), curbura dorsala concava anterior = the anterior concave dorsal curve, vertebra 12 dorsala = the 12th dorsal vertebrae, vertebra a 5-a lombara = the fifth lombar vertebrae, osul sacru = sacrum, coccis = coccyx.
Curbura anterioara a vertebrelor cervicale = anterior curve of the cervical vertebra, curbura posterioara a vertebrelor toracice = posterior curve of the thoracic vertebra, curbura anterioara a vertebrelor lombare = anterior curve of the lombar vertebra, curbura posterioara a portiunii sacrococcigiene = posterior curve of the sacrococcygean part.
Copyright © 2025 - Toate drepturile rezervate